The rare case of six canals – Dr Byron Tsivos (DDS MSc Endodontics)
Featured Products Promotional FeaturesPosted by: Dental Design 4th December 2018

Dr Byron Tsivos (DDS MSc Endodontics) is a specialist endodontist at The Square Dental Referral Clinic in Isle of Man. Dr Tsivos received his MSc in Endodontics in 2008 from the UCL Eastman Dental Institute, and is an active member of both the British and European Endodontic Societies. Here, he presents a rare case in which six canals were identified and treated in the LL6.
Patient complaint
The patient was referred by a local general dental practitioner with a complaint of recent episodes of pain and swelling of his LL6 exacerbated by biting. Nothing of clinical note was associated with the patient’s medical history and he was a regular attender.
Six canals were identified and treated in this case. Usually mandibular first molars have three to four canals.[i]It has also been postulated that 3% of the first lower molars could have a third mesial or distal canal.[ii]In this case a third canal was identified and treated both mesially and distally and the occurrence of the latter finding in a single tooth is extremely rare with only three case report publications.[iii],[iv],[v]
Clinical examination
During the initial consultation the LL6 was not responsive upon sensibility tests using Endo-Frost (COLTENE) and an Electric Pulp tester, and was found tender on percussion. A fistula associated with the soft tissues was noted buccally and some tenderness on palpation, while tooth mobility was within normal limits. The preoperative periapical radiograph that was taken revealed periradicular radiolucencies associated with the roots of LL6 (see Figure 1).

Fig 1
Diagnosis
Based on a provisional diagnosis of chronic apical periodontitis with acute exacerbation, the following options were given to the patient: non-surgical root canal treatment of LL6 subject to its restorability assessment; and extraction of LL6. After discussing the pros and cons of each the patient opted for endodontic treatment.
Treatment pathway
At the following appointment the LL6 was found restorable under high magnification after the removal of the old filling and carious tissue. The tooth was isolated with a heavy-duty rubber dam (COLTENE) and a cotton pellet immersed in NaOCl 3% was used to disinfect the rubber dam, access cavity and clamp prior to commencing treatment.
Then, with the use of a DG 16 endo probe, four canal orifices were noted initially (two mesial and two distal). A hand file was used to negotiate the canals and scout. After further inspection at higher magnification and the use of X3 Smart EMS tip troughing at the mesial embryomental grooves, a third mesial and a third distal canal were identified. All six canals were prepared at 0 reading with stainless steel hand files to a size 15 and then with HyFlex™CM NiTi files by COLTENE (500 rpm 2.5 N.cm Torque) to 0.4 size 30. HyFlex™CM files have been my rotary instruments of choice for over six years now due to their many superior features, including controlled memory and exceptional fatigue resistance.
Another critical point is that these files can be precurved and accessing difficult canals is really easy now. In the past I had to enlarge the access cavity and stress my rotary files in order to treat mesiobuccal canals of lower second or third molars or upper maxillary second or third molars. That’s not the case with HyFlex™CM files – and what’s more, they can be returned to their original shape with heat treatment. This gives me great confidence that I can reinsert the instrument back into a highly curved canal. Further to this, HyFlex™CM files have been shown to be superior on apical extrusion of debris and have less dentinal cracks than other files. They also eliminate transportation problems and retain original anatomy in a way that I have never seen with another instrument.
Once the root canal system was prepared, irrigation was carried out using NaOCl 3% and EDTA 17% solutions before passive ultrasonic irrigation and dynamic master cone agitation was used to agitate the heated to 60˚ C irrigants.
Final obturation of LL6 was performed with continuous wave of condensation technique and the access cavity was sealed withMIRIS®2, a multi-shade nano-hybrid compositeby COLTENE (see Figures 2,3 and 4).

Fig 2
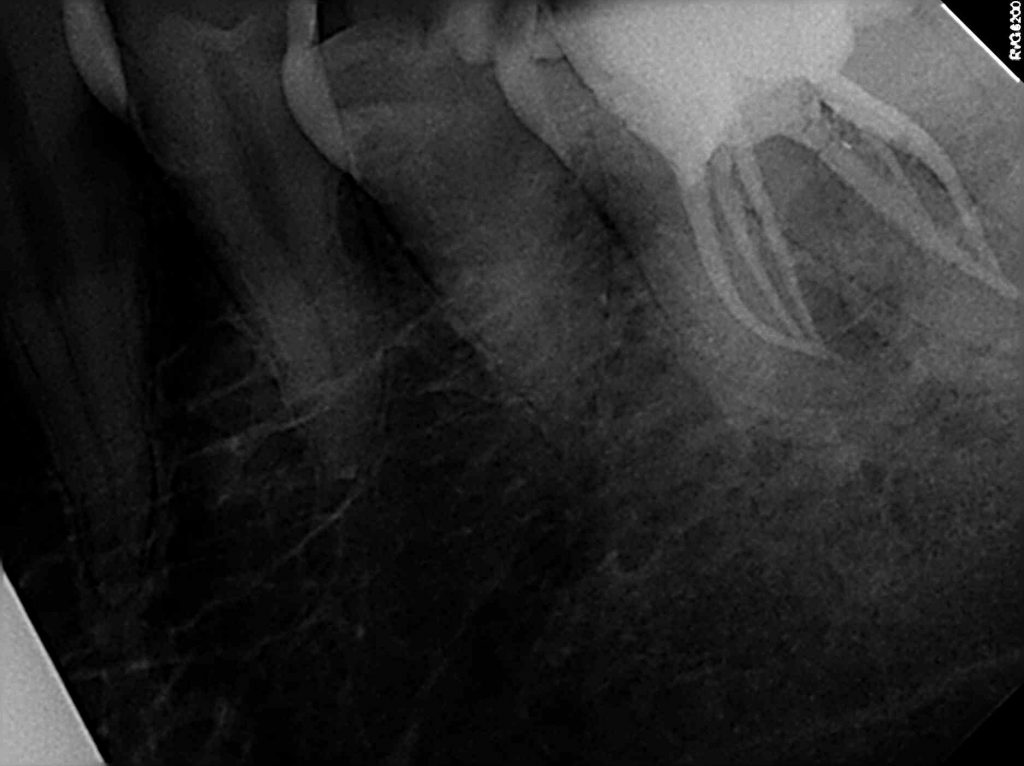
Fig 3
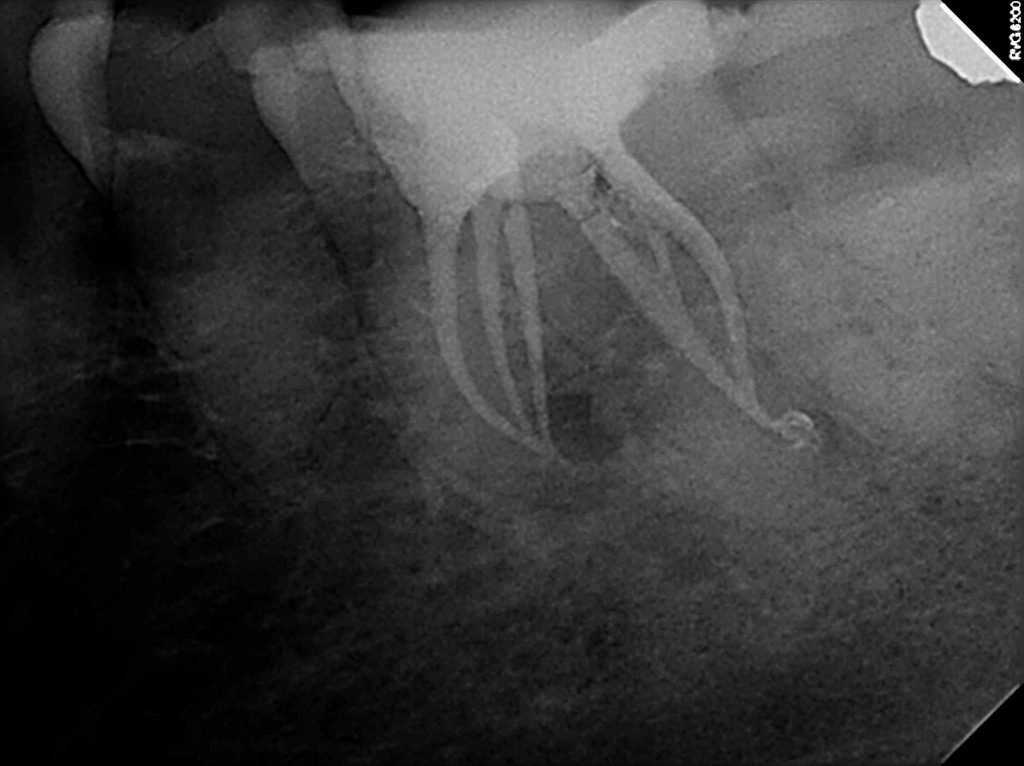
fig 4
Outcome
A week after treatment, the patient was reviewed and the LL6 was found to be symptom free with a good endodontic prognosis. As such, he was referred back to his practitioner for a crown restoration and his routine care.
To find out more visit www.coltene.com, email info.uk@coltene.comor call 01444 235486
[i]F. J. Vertucci, “Root canal anatomy of the human permanent teeth,” Oral Surgery Oral Medicine and Oral Pathology, vol. 58, no. 5, pp. 589–599, 1984.
[ii]H. A. Ahmed, N. H. Abu-Bakr, N. A. Yahia, and Y. E. Ibrahim, “Root and canal morphology of permanent mandibular molars in a Sudanese population,” International Endodontic Journal, vol. 40, no. 10, pp. 766–771, 2007
[iii]E. S. Reeh, “Seven canals in a lower first molar,” Journal of Endodontics, vol. 24, no. 7, pp. 497–499, 1998.
[iv]J. L. Ryan, W. R. Bowles, M. K. Baisden, and S. B. McClanahan, “Mandibular first molar with six separate canals,” Journal of Endodontics, vol. 37, no. 6, pp. 878–880, 2011
[v]F. R. F. Alves, I. N. Rôças, B. M. Almeida, M. A. S. Neves, J. Zoffoli, and J. F. Siqueira, “Quantitative molecular and culture analyses of bacterial elimination in oval-shaped root canals by a single-file instrumentation technique,” International Endodontic Journal, vol. 45, no. 9, pp. 871–877, 2012.
No Comments
No comments yet.
Sorry, the comment form is closed at this time.